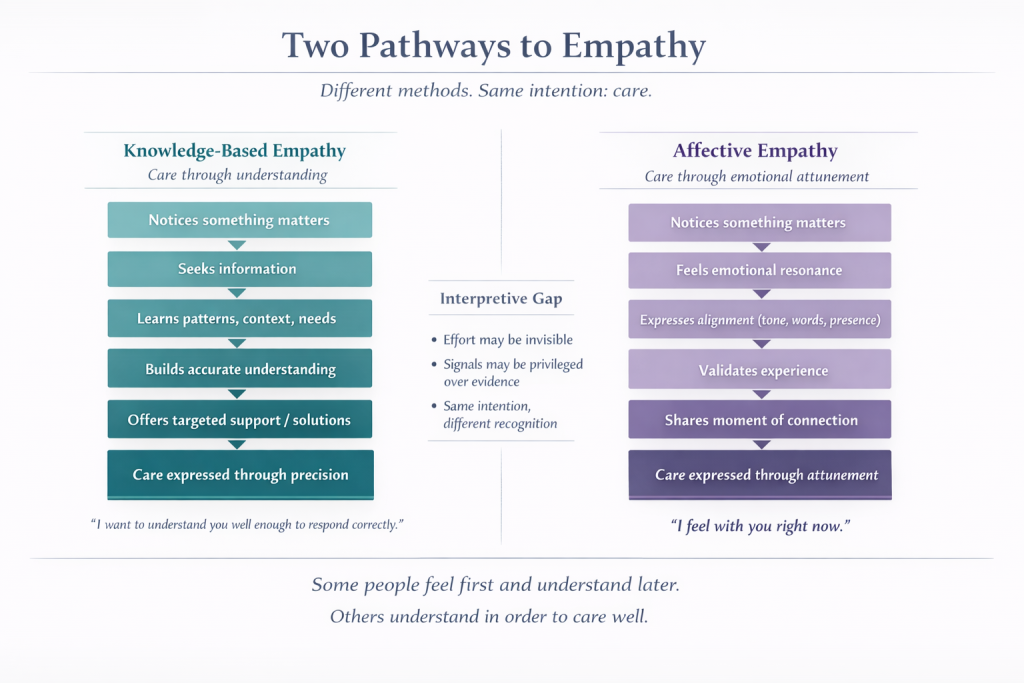
Some people build empathy through understanding. Others express it through feeling.
Autistic clients often construct empathy through knowledge acquisition. They learn about people in order to care for them accurately. They research health conditions, interests, work contexts, family dynamics—anything that might shape a person’s experience. This system asks:
Do I understand you well enough to respond correctly?
Neurotypical norms tend to privilege affective resonance—feeling with someone in the moment, often without requiring explicit knowledge. This system asks:
Do I feel with you right now?
Neither approach is inherently superior. But only one is consistently recognized as “real empathy.”
When people talk about empathy, they often treat it as an immediate emotional experience. Something spontaneous, visible, and shared in real time. A look of concern. A soft tone. The right words at the right moment.
This is what tends to register.
But for many autistic people, empathy is not primarily immediate. It is constructed.
It begins with noticing that something matters to another person. From there, it moves into information gathering. Sometimes this happens quickly, sometimes over time. Patterns are tracked. Preferences are remembered. Context is built. Understanding is refined.
Care is expressed not through immediate emotional alignment, but through accuracy.
Not guessing. Not approximating. Learning.
Learning about what matters to a person so it can be taken seriously.
And learning the person themselves so responses can be accurate, not assumed.
This form of empathy is effortful.
It requires:
In many cases, it involves doing more—not less—than what is socially expected.
But that effort is often invisible.
Because it does not always produce the signals that are recognized as empathy—facial expression, tone, immediate validation—it can be misinterpreted as distance, analysis, or even lack of care.
At the same time, affective signals are often treated as sufficient evidence of empathy, even when they are not grounded in deeper understanding.
This creates a predictable mismatch.
A person who has taken time to understand someone in detail may respond with:
And this can be received as:
Meanwhile, a response that signals emotional alignment—without necessarily incorporating detailed understanding—is readily accepted as empathic.
Consider a common moment:
Someone shares that they’ve just been diagnosed with a chronic condition.
An autistic person responds by reading about the condition, learning common challenges, and coming back with specific, relevant suggestions—things that might actually reduce difficulty or improve quality of life.
The response they receive is:
“I just needed you to listen.”
What is visible in that moment is not the care that was built.
Only that it did not match the expected form.
The care was there. The format was wrong.
The result is not simply misunderstanding.
It is a difference in what counts as evidence of care.
Both pathways begin in the same place: Something about this person matters.
From there, they diverge:
One prioritizes precision.
The other prioritizes attunement.
Both are valid. However, they are not equally recognized.
When knowledge-based empathy is not recognized as empathy, several things happen:
Over time, this can lead to:
Not because empathy is absent—but because the criteria for recognizing it are narrow.
Disclosure is often treated as information sharing.
For some, it is an invitation to understand.
This difference in how empathy is constructed does not only shape how care is offered.
It also shapes what is expected in return.
Many autistic clients describe a similar assumption:
If I tell someone something important about me—a diagnosis, a condition, a constraint—they will want to understand it.
They will look it up. They will learn what it means. They will adjust based on that understanding.
That is what care requires.
This expectation is not arbitrary.
It is based on what they themselves would do.
But often, that is not what happens.
The other person may:
From the outside, this can look like indifference. Or lack of care. Or unwillingness to understand.
But within a system that prioritizes affective empathy, the expectation is different.
The signal of care is the response in the moment, not the accumulation of knowledge over time.
This creates a second layer of mismatch.
Not only is knowledge-based empathy misread when offered—
it is often not reciprocated when expected.
The result is a specific kind of disappointment:
What is being violated is not just expectation.
It is a model of care.
Some people feel first and understand later.
Others understand in order to care well.
If we only recognize the first as empathy, we will consistently misread the second.
And we will also fail to meet it when it is expected in return.
Empathy is not only what is felt in the moment.
It is also what is built, over time, in the effort to understand someone accurately.
"*" indicates required fields